
Educators
10
May
2019
Lava Paper: Dramatic Game Paper make learning handwriting more fun
Pediatric OTs or parents: If you’re working with a child who is highly intelligent but has poor handwriting and one of the reasons is that they are bored/don’t care about sizing rules….this “lava paper” (game paper) is for you.
Category: Activities, Clients/Consumers, Current OT Students, Educators, Occupational Therapy, Parents, Therapists | Comments: none | Tags: Activities
9
Aug
2018

The importance of validating feelings
 I haven’t posted about OT in a loong time here! But this situation arose the other day and it got me reflecting.
I haven’t posted about OT in a loong time here! But this situation arose the other day and it got me reflecting.
My friend and I were leaving a restaurant.
A white-haired woman was slowly headed towards the sidewalk in front of the restaurant. She had the panicked look of someone who is scared of falling. Another lady was holding her hand, helping steady her as they walked. A white-haired man waited at the curb for them.
As the unsteady woman reached the curb, requiring her to step up, she hesitated.
The man at the curb said to her, neutrally but with slight impatience: “It’s not a mountain.”
As I walked past, I chimed in: “It FEELS like a mountain.”
The woman instantly cried out, “YES! THANK YOU!” in a relieved tone. She felt validated/seen.
I am about to start teaching psychosocial OT/mental health to incoming Occupational Therapy Assistant (OTA) students, for the third time now, and one thing we circle back to again and again is validation of feelings of their clients.
Yes, maybe a curb is not a mountain, maybe other people have it worse, blah blah blah. But people crave validation. Especially people in pain or fear. It doesn’t mean we are agreeing with them. It just means we hear them, see them. Often, once a person feels validated, they’re then more willing to hear alternative points of view, or to move on.
The day I first introduce validation as an important component of therapeutic use of self with clients, I have them watch this brief clip from the incredible animated movie “Inside Out.”
In this sweet, sad clip, we quickly see the outcomes of invalidating versus validating feelings. Even children can understand the concept once it’s discussed using that clip as an example.
I love the concept of “therapeutic use of self” and address it in a blog post here as well: https://missawesomeness.com/therapeutic-use-of-self-in-ot
Category: Current OT Students, Educators, Occupational Therapy, Prospective Students | Comments: none
10
Aug
2016

Easy Ways to Teach Your Child Problem-Solving Skills

Does your child get upset easily over small and easily fixable things, like a ball rolling under a table? It may be because he doesn’t realize he has any power to fix the problem. Luckily, you can teach him to feel more empowered. I introduce to you the PSST Method!
Download the PDF of this here: The PSST! Method: Teach Your Child How to Problem Solve
Or just read on.
The PSST! Method: Teach Your Child How to Problem Solve
Children who feel confident in their problem-solving abilities can better tolerate and handle unexpected events. All children of any age can benefit from learning problem-solving skills. Adjust your language or extent of experimentation based on your child’s age/ability/tolerance level. The steps stay the same. (Ideally, use them all in order. But using any is great.)
SAMPLE PROBLEM: Young John’s ball just rolled under the couch. John scrunches up his face, ready to cry. Daddy jumps up to go grab a broom handle and solve the problem.
WAIT! John needs to learn the steps BETWEEN the problem and a successful solution.
- Pause. Just briefly. See if the child will attempt to problem-solve. If not, proceed to step two. Eventually, your child may make the attempt.
- Frame the Problem. “Wow, the ball rolled under the couch, and we can’t reach it.” You can also provide “emotion” and “help” words. “Your face is turning red and you look really frustrated. You can say, “Please help me solve this problem.”
- Play “Dumb.” Whether you instantly have a solution or not, you can pretend you’re not quite sure what to do. Crinkle up your forehead and look thoughtful. “Hmmm….”
- Think Out Loud. Most adults problem-solve in their heads. If you can role-model the problem-solving process, you’re giving him valuable insight, and showing that it’s not magic. “The ball’s is under the couch. We have to get it out somehow…maybe we can try…” With an older child, you can ask them if they have any ideas.
- See What Happens. You may know that your hand won’t fit or his arm can’t reach, but he doesn’t. When it’s feasible to experiment (not a safety hazard or massive inconvenience), try it out. He learns a lot more that way. “Let’s see if your arm is long enough. Can you lie down and reach for it?”
- Repeat Steps # 4 (Think Out Loud) and #5 (See What Happens), until problem solved. “That didn’t work because the ball’s too far away, will my hand work? …No, too big. Hmm, maybe something small but long to help us get the ball.. see if this will work…no….hmm…let’s see if we can find something…oh, let’s try a broom handle!”
- Frame the solution. “The ball rolled under the couch and we were really frustrated and we didn’t know what to do. But we tried lots of ways to solve the problem and now we have our ball back. We are great problem-solvers!”
Repeat this process regularly. As he becomes more proficient, you can take more of a back seat to the problem-solving process.
Bonus: Consider sprinkling “What If’s?” into your conversations/play time. “We solved that problem! What if the ball landed in a tree? Or this hole? Or under the bed?” Talking is great, acting it out is even better. Play a game called “Problem-Solving Superheroes” where you deliberately practice these kinds of things.
Good luck – let me know how it goes!
PS: This method may seem obvious to you – but many caregivers would benefit from the reminder.
Category: Activities, Clients/Consumers, Current OT Students, Educators, Occupational Therapy, Parents, Therapists | Comments: none | Tags: Activities
20
Jul
2016
Interested in practical adaptive equipment design?
See flyer here:
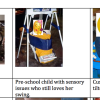
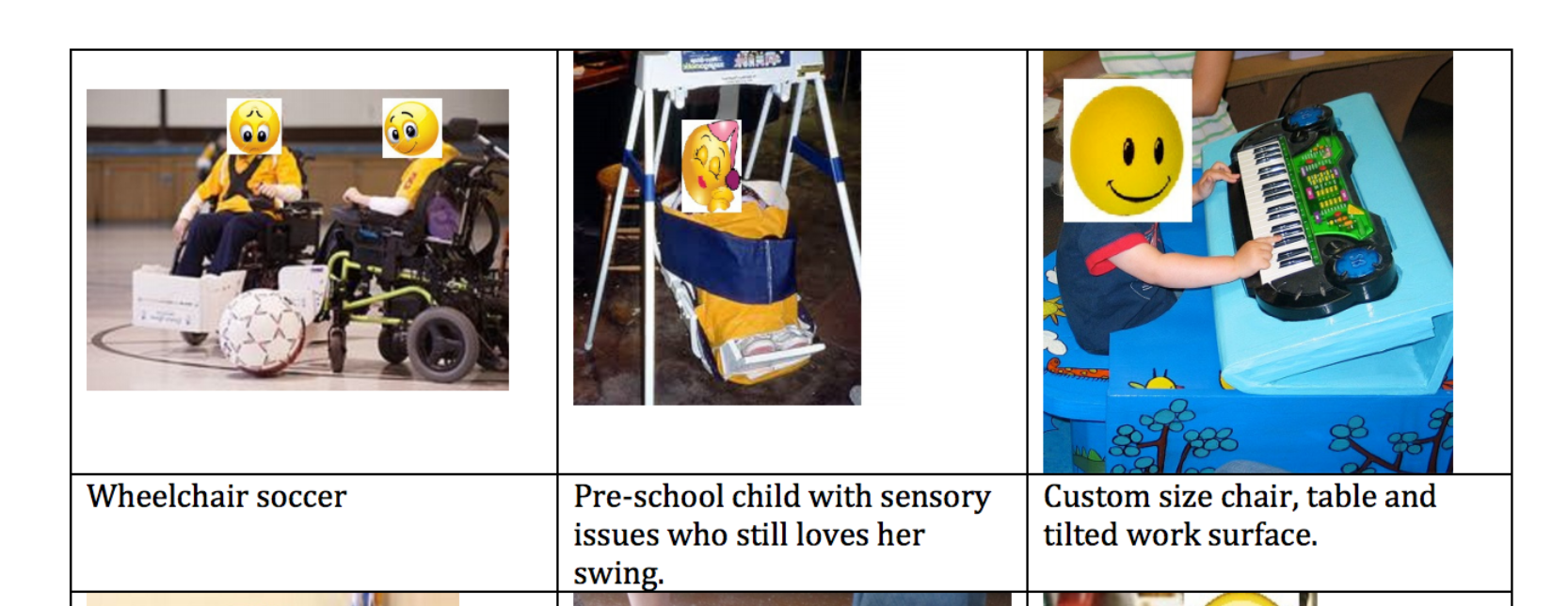
Homemade Customized Adaptive Equipment
My lovely friend Beth has been working on practical adaptive equipment – creating it at a fraction of the cost of commercial design. I copied the following text from the flyer: “I want to customize or build adaptive items for children with special needs. My dream is to have a workshop where families, teachers and designers can meet. Footrests, booster seats and supportive seats can be purchased from special needs catalogs but they are generally hundreds of dollars. I make most items out of extra strong cardboard, plastic, fabric and foam. They are inexpensive, light-weight and last a long time. I took cardboard construction classes at the Adaptive Design Workshop in New York City. The founder, Alex Truesdell, won a McArthur Award for her work. Many students who take the class are interested in starting their own workshops. It really helps to have experience building things.
What products do your kids need most? What features do you need that you can’t find? What do you want but can’t afford? I would love to hear your ideas. I’m not in business yet. I just learned that product liability insurance costs a minimum of $3500 per year. (On top of general liability insurance.) I may have to find or create a position at an existing company or organization that already serves the special needs population. Apparently, the price of insurance is stopping many of my fellow students. Connections are welcome!”
Her contact information is provided in the flyer. If you have any interest in adaptive design, or want some ideas or to know more about her work, you should definitely connect with her.
Category: Current OT Students, Educators, Occupational Therapy, Parents, Therapists | Comments: none
21
Mar
2016
The ethical issue of productivity in healthcare
I haven’t blogged in a loooong time and as I was going through old files, I found something I had written about “productivity” within healthcare and the ethical issues I have with it, as an occupational therapist.
Essentially, many hospitals/clinics/settings have a set amount of “productivity” (billable units of time, typically in 15 minute increments, and usually only gotten during client treatment time) that each therapist is expected to get each day. Now, of course productivity can be a good thing in that obviously we want occupational therapists treating clients versus sitting around eating bon-bons, but the reality is that most therapists are already rushing around all day, doing their best to see all their clients, do paperwork, schedule things, collaborate, etc. What I’ve found is that unrealistically high productivity standards tend to lead to ethical dilemmas.
Here’s an example I give, which I experienced during fieldwork in 2009:
I am working on a locked geriatric psych ward. I just finished up an occupational therapy treatment session with a very mobile male who frequently gets aggressive (throwing chairs in hallways and such). He has a short fuse and if he gets stressed/frustrated, he escalates. I’m supposed to meet productivity units and my time is very limited for the rest of the day. As I am walking out of his room where he has gotten into bed, he asks me for a drink of water. Patients can’t get it themselves. I hesitate and the following goes through my brain:
Scenario 1: I get him the drink of water as requested. It will require me heading down a long hallway and navigating multiple people who want my attention, tracking down a nurse for a key, going into a room and getting the water if there are even cups in supply, finding the nurse to return the key, and walking back. He may expect that it’s a simple request, but even if everything goes smoothly, it could take 5 minutes, and possibly closer to 15. I will lose at least one precious, precious unit, but at least he got a need meet as soon as possible and on first request, which means he will -more likely – stay calm. (Why it takes so much work to get water is a separate issue not addressed here!)
Scenario 2. Worst case scenario plays out. I don’t want to lose my productivity so I let him know I have to run but I will ask a nurse as I am headed out. It may be true, but I know full well the chances are extraordinarily high, thanks to strained resources, that the nurse will take mental note and get to it when she can, which may take a while, and that in the meantime, every time anyone walks by his room, he will ask whoever that is again, who will say they will tell his nurse, and he will become increasingly frustrated. Here he is asking for the simplest and basic of needs to be met and nobody will help him. He will escalate to violence, throwing chairs in the hallway as he tends to do. (There’s only one hallway/entrance – no way to get out if he’s blocking it) All other residents will be stuck inside their rooms as area staff deal with this. Now there are six people focusing on de-escalation. In the meantime, patients are stressed, nurses run behind on meds, and I may be stuck somewhere, having to wait until the coast is clear. Now all the employees have lost productivity, quality of care is suffering as now all the poor patients have to deal with this. And it’s certainly not fun for the agitated patient, either. And even if I had already left the area so it didn’t affect MY productivity, it was certainly horrible for those left behind.
IF I DO SCENARIO 1: I get him the water, no escalation, everything stays more or less on track, and I have lost a unit with no good reason (in director’s eyes), which I may get scolded for later. The director doesn’t appreciate hearing “Well yes I didn’t get that unit but it’s because if I didn’t get him his water then X would occur then Y then Z so really I saved units.”
IF I DO SCENARIO 2: I don’t get him the water. I potentially get my productivity unit. The department is happy. If he didn’t end up escalating, I’m happy I did in fact get my unit, but I still feel guilty that I didn’t help him. If he did end up escalating because of not getting his water fast enough, I feel absolutely hideous.
==========
I quickly learned through fieldworks that I am not able to handle a job with productivity units. I would have been fired quickly. I get too stressed out about it. Too much worst case scenario thinking and too hard of a time saying no (or if I do say no, I obsess). I need to work on those issues, I do know that!
There are tons of very ethical therapists who work quite successfully in placements with productivity, obviously. I always wish I could be inside their heads to see what it would feel like to not go into worst case scenarios or always feeling bad about sometimes having to say no. Like in the situation above. I obviously went into worst case scenarios.
Luckily the American Occupational Therapy Association (AOTA) has been addressing the issues of productivity and ethics in our field – helping ensure that productivity standards are realistic and don’t lead to increased likelihood of ethical dilemmas, for example.
30
Nov
2015
My occupational therapy capstone project is complete!
I wrote mine on “Increasing Awareness and Acceptance of Children with Disabilities Using Picture Books.” My Capstone Paper
I write about the importance of awareness and acceptance of children with disabilities, and how children’s picture books can serve as a form of disability awareness, which can promote acceptance, and therefore social inclusion…which ultimately leads to increased participation in occupation, which is the whole point of occupational therapy.
In addition, I talk about how OTs should consider incorporating picture books into their practice, and also how OTs should consider writing their own children’s books! It furthers the Centennial Vision, is a form of occupational justice, utilizes our unique talents, is in alignment with the Framework-III, and also has bonuses, on the business side of things. So far only four OTs that I know of have written five children’s book that have OT in them or even disabilities at all. Karen Jacobs, famous OT of the world, has written two of them. I want to be in the top ten. 🙂 Of course books about children with disabilities exist, but not enough of them, especially high quality ones.
Business wise, selling high-quality children’s books that exist already is a way to make a few extra dollars. And selling, giving away, or recommending them, especially if they are your own books, can be a value-added service, promoting satisfaction and loyalty. They are great for marketing. And if you write your own, especially if done as an e-book, you can make some money…well assuming it’s successful. Although to warn you, children’s books are hard to write well, and illustrations are quite costly.
To learn more about the process, read my capstone manuscript…the process etc is near the end, you can find via Table of Contents.
Use the Contact Me button on my website or email me…my name karendobyns, on gmail.com, if you want to say anything, because I just switched servers and the spam is out of control. I have over 2,000 comments and I won’t see yours…I have to get it fixed. Ugh.
Anyway….I got an A on my capstone YAY and after the presentation I give in 45 minutes through GoToMeeting (I think that’s the name), I am done with all but a single reflective post worth 1 point. 🙂 Post-professional clinical doctorate of occupational therapy (OTD), here I come!
9
Nov
2015
Cadillac OT versus Reality OT
A wonderful occupational therapist/educator wrote the following forum post on our OTD forum (we are getting our post-professional clinical doctorates in OT). I asked her permission to post it because it resonated. What we learn in OT school and what we discover in the real world are two different things – but we have to remember in the real world that what we learned in OT school is still a valid and burning flame within us we must nurture and allow to grow.
“I remember something that one of my professors once said: “What you get in OT school is the ‘Cadillac version of OT.” I didn’t really understand it at the time, but the idea has stuck with me and I have certainly seen it in my own career. A lot of what we learned in school is how it should be, but not necessarily how it is currently. But we needed to learn it that way if there is any hope of changing things going forward. Each of us are then charged with holding on to pieces of the “Cadillac version” that fit within our practice, working to change things in practice to fit more of that in, and adapting to what we cannot change.
I try to make my teaching fit that approach. We emphasize occupation-based practice a lot in our curriculum, and we do teach preventative care and wellness, which aren’t necessarily reimbursed or even being practiced where our students complete their fieldwork. But some of our students have been able to fit these things into the otherwise very limited medical model at their sites, and others have the desire to find practice settings in the future that will allow them to use these skills.” – J.D.
4
Apr
2015
Can observing a client in one context allow us to predict ability in another?
I created this scenario to explain how, for example, assessing “Mary’s” ability to get ready in the morning (her “occupational performance”) can tell me a lot about her likely performance in making a simple meal.
(A modification of this would be great to use with OT/OTA students in the classroom or on fieldwork. Sharing how Mary does in her morning routine, then asking them to predict what she would be like in the kitchen.)
Mary is a 75-year-old woman who wants to be able to independently make a simple meal, while using hip precautions, her walker, and energy conservation techniques. She is currently in inpatient rehab. If we [OTs] work with her during her morning routine , even if we haven’t seen her in the kitchen yet, we will learn valuable information to predict how she would do in the kitchen. We may see she is forgetting to use- or doesn’t understand- her hip precautions. We may see that she is inefficient in her method, walking back and forth across the bathroom to get one item at a time. That she sequences tasks incorrectly, putting on makeup then realizing she hasn’t washed her face. That she is unsafe, with seemingly no awareness of fall hazards or an ability to remember to turn off her curling iron. All of these components will demonstrate to the OT that she may not be ready to safely make a meal by herself that involves anything that needs to be turned off, and that she may need items grouped together for efficiency reasons, such as keeping the peanut butter, jelly, bread, and a butter knife all in one area. She may also benefit from a written or visual list of instructions. We haven’t even seen her in the kitchen yet, but by watching her in the bathroom, we already have information that will guide our intervention and possibly fill in some of the blanks on an assessment tool. There are many safety similarities between getting ready in the morning and making a meal, as it pertains to slippery surfaces, heated objects, sequencing, underlying skill deficits both physically and cognitively, etc.
*I’m using more laymen terms here for easier understanding, but in medical documentation I would use more professional terminology
*Born out of a discussion in one of my post-professional OTD classes, involving assessment of various occupational performance areas.
(Prediction of occupational performance in varying activities of daily life (ADLs)
Category: Educators, Occupational Therapy | Comments: none
14
Feb
2015
Remembering our upbringings affect our expectations of clients
Just thinking out loud/reflecting here. 🙂 I really enjoyed reading the following Facebook post by F.C. on the group page, “Pediatric Occupational Therapists”. (I recommend joining this group, a lot of high-quality information and resources.) I enjoy outside-the-box thinking and creativity, and at times I felt guilty trying to reconcile my work with some of the more rigid academic necessities. I did have a typical schooling so I understand “normal” expectations, but I think more like F.C.!
“I went to a very small alternative school from 1st grade through high school that really emphasized individuality and creativity. It was a wonderful place to be and we learned a lot of great life skills, but there was no OT and no one was too concerned with typical development. Fast forward 20 years and I am at my first fieldwork placement at a peds clinic, working with a little boy who was coloring. He was having a great time and using a bunch of different colors and free form drawing before he filled in the shapes… My supervisor (who is lovely) walked in and called him out on not coloring properly – oops! I had no idea up to that point (as a 30 year old) that coloring is usually supposed to be one color, fill the whole area systematically, etc. I thought this kid was doing great! It was an interesting reminder that my upbringing is always going to affect the way I see things and the way I treat. I’m still not sure of everything kids are “supposed” to be doing at certain ages, except out of text books, which don’t give us much.”
8
Feb
2015
Controversy: Patient versus Client versus Consumer?

Patient, Client, or Consumer? In occupational therapy and other healthcare fields, there is a semantic controversy over what us therapists/the public should be calling those who utilize occupational therapy services. Depending on the label used, we get a different feel for the relationship between therapist/person.
My friend, a psychologist, told me she likes to use the word “patient” because it came from Latin and means “one who suffers,” and she feels the people who see her are there because they are suffering. Some therapists prefer “client” as they feel “patient” has more of a superior-inferior feel, as well as a “medical model” feel, and many OTs feel we need to be more encompassing. Other therapists prefer “consumer” because it seems to have a more neutral connotation. I’m sure there are plenty of other reasons for the different labels. Some therapists feel very passionately about the “appropriate” label, others don’t really care, others use them interchangeably. I think there may be an even better label out there. Hmm. So I just asked my pediatric therapist friend what she calls the people she sees, and she said with a shrug, “child.” I loved that answer! Maybe that’s the best one of all. 🙂
What do you think? Patient, client, or consumer?